If you bill for audiology services, 2026 brought changes you simply cannot ignore. CMS overhauled the entire hearing device CPT code structure for the first time since 1993. Thirty-three years of legacy codes are gone. Twelve new ones took their place. On top of that, the conversion factor shifted, the efficiency adjustment hit most non-timed diagnostic codes, and MIPS rules got updated again.
Whether you run a private audiology practice or manage billing for a multi-provider ENT group, this guide breaks down 2026 audiology fee schedule code by code and what your team needs to do to keep claims clean.
The 2026 Conversion Factor and What It Means for Your Practice
CMS published the Calendar Year 2026 Medicare Physician Fee Schedule Final Rule on October 31, 2025. It went live January 1, 2026. The rule sets two separate conversion factors.
For audiologists in qualified Advanced Alternative Payment Models, the rate is $33.57. For everyone else, which is the vast majority of audiology practices, the rate landed at $33.40. That is a 3.26% increase over the 2025 rate of $32.35, reflecting a statutory baseline update of 0.25% plus a one-time congressional increase of 2.5%, with budget-neutral RVU adjustments layered in.
Most non-time-based audiology procedures were subject to a negative 2.5% efficiency adjustment in the 2026 final rule.
That adjustment applies to codes like comprehensive audiometry (92557), speech testing (92556), tympanometry and immittance codes, OAEs, and vestibular testing.
The increase in the conversion factor does not offset the decrease in efficiency. For many commonly billed audiology codes, the net change in reimbursement is either flat or slightly negative once you run the actual math.
| About 15% of American adults report some degree of hearing loss according to the National Institute on Deafness and Other Communication Disorders. That is roughly 40 million people. Hearing loss is the third most common chronic physical condition in the United States, behind hypertension and arthritis.
Yet hearing aid adoption rates hover around 20% of those who could benefit. Part of that gap is cost. Part of it is access. The modernization of the hearing device CPT code set is one piece of a larger effort to improve how audiology care is described, valued, and ultimately reimbursed outside of Medicare. For commercial insurance billing, the new code structure is an actual opportunity to renegotiate your fee schedules. The old six codes from 1993 made it nearly impossible to capture the clinical complexity of a 60-minute, cognitively aware candidacy evaluation with real-ear measurement. The new codes do exactly that. Use them to make the case when you are at the table with commercial payers. |
Without careful code-by-code analysis against your specific payer mix and patient volume, you could easily project 2026 revenue incorrectly.
What Medicare Covers for Audiology in 2026
Medicare covers audiology services under Section 1861(s)(3) of the Social Security Act as “other diagnostic tests.” These are paid under the Medicare Physician Fee Schedule. In hospital outpatient settings, they are paid under the OPPS instead.
Medicare covers diagnostic audiology services. It does not cover hearing aids or the professional services directly associated with the fitting, selection, and management of hearing devices. That exclusion is written into Section 1862(a)(7) of the Social Security Act and has been there since Medicare was created in 1965.
One access rule that has been in place since January 2023 still applies in 2026. Patients can self-refer to an audiologist once every 12 months for certain diagnostic tests for non-acute hearing conditions without a physician order. This applies specifically to direct access for diagnostic tests personally furnished by the audiologist. Tests for disequilibrium or imbalance still require a physician order.
2026 Medicare Fee Schedule: Diagnostic Audiology Rates
The table below shows the national non-facility Medicare reimbursement rates for commonly billed diagnostic audiology CPT codes in 2026.
Rates reflect the $33.40 conversion factor and post-efficiency-adjustment RVUs. Actual payments vary by geographic locality, so check your specific MAC fee schedule for the exact rate in your area.
| CPT Code | Service Description | 2025 Rate (Non-Facility) | 2026 Rate (Non-Facility) |
| 92552 | Pure tone audiometry, air only | $38.82 | $40.42 |
| 92553 | Pure tone audiometry, air and bone | $46.90 | $49.10 |
| 92555 | Speech audiometry threshold | $29.44 | $29.73 |
| 92556 | Speech audiometry with speech recognition | $45.61 | $46.43 |
| 92557 | Comprehensive audiometry (92553 + 92556 combined) | $35.26 | $35.74 |
| 92567 | Tympanometry | Varies by locality | ~$16.00 |
| 92568 | Acoustic reflex testing | Varies by locality | ~$10.00 |
| 92550 | Tympanometry and acoustic reflex thresholds | Varies by locality | ~$22.00 |
| 92585 | Auditory brainstem response (ABR), comprehensive | Varies by locality | ~$100.00 |
| 92587 | Otoacoustic emissions, limited | Varies by locality | ~$33.00 |
| 92588 | Otoacoustic emissions, comprehensive | Varies by locality | ~$60.00 |
| 92540 | ENG/VNG comprehensive battery (vestibular) | Varies by locality | ~$175.00 |
Note: Rates marked as approximate reflect the post-efficiency-adjustment RVU conversion and vary by MAC locality. Always pull your specific rates from the CMS Physician Fee Schedule Look-Up Tool or your MAC portal before finalizing projections.
A few things worth noting about this table. The comprehensive audiometry code 92557 is significantly lower than the sum of its component codes 92553 and 92556 because it carries a combined RVU, not two full individual RVUs. If you are billing 92553 and 92556 separately when all components of a comprehensive evaluation were completed, you need to stop. That is unbundling. NCCI edits catch it, and OIG audits specifically flag this pattern with an estimated 15% error rate in sample audiology claims.
Also note that 92557 should be reported only after you have completed all required components. That means pure tone air and bone conduction, speech reception thresholds, and speech recognition testing. If you only performed part of the battery, use the component codes that match what was actually done.
12 New Hearing Device CPT Codes Replace 33-Year-Old Legacy Codes
This is the change that affects the most audiology practices and has created the most confusion heading into 2026. Effective January 1, 2026, CPT codes 92590 through 92595 were deleted. Gone. Replaced by 12 new codes that better reflect how audiology care is actually delivered today.
The old codes were written in 1993 when hearing aids were analog. They did not capture cognitive assessment during the candidacy process. They did not account for verification of real-ear measurements. They did not reflect the complexity of digital device fitting, remote programming, or the range of patient-specific factors that modern audiologists address.
The new codes are organized around four stages of hearing device care: candidacy evaluation, device selection, fitting and follow-up, and verification services. Most of the new codes are time-based, which is a significant structural change from the old system.
Here is a breakdown of all 12 new codes.
Stage 1: Candidacy Evaluation (92628 and 92629)
| CPT Code | Service Description | Time | Medicare Covered? |
| 92628 | Hearing aid candidacy evaluation; first 30 minutes | Base code, 30 min | No |
| 92629 | Hearing aid candidacy evaluation; each additional 15 min (add-on) | +15 min | No |
Code 92628 covers the assessment of whether a patient is appropriate for amplification. The service includes reviewing audiologic function test results, assessing speech-in-noise performance, discussing candidacy results with the patient, counseling on treatment options, and producing a written report. When clinically appropriate, it also includes assessment of cognitive and communication status.
92629 is the add-on code. You bill it for each additional 15-minute increment beyond the initial 30 minutes of candidacy evaluation work.
These codes are time-based and follow the half-plus-one rule. You need at least 16 minutes documented to bill 92628. For each unit of 92629, you need at least 8 minutes beyond the full 30-minute base.
Do not bill 92628 or 92629 on the same date as 92631, 92632, 92636, 92637, or 92642. They also cannot be billed alongside 92622, 92623, 92626, or 92627 if performed on the same ear.
Stage 2: Device Selection (92631 and 92632)
| CPT Code | Service Description | Time | Medicare Covered? |
| 92631 | Hearing aid selection services, unilateral or bilateral; first 30 min | Base code, 30 min | No |
| 92632 | Hearing aid selection services; each additional 15 min (add-on) | +15 min | No |
Selection services include reviewing audiologic results and candidacy evaluation findings; assessing the patient’s visual and dexterity limitations; evaluating psychosocial factors; determining device type and output requirements; selecting signal-processing strategies and additional features; and discussing device recommendations in a written report.
The AMA issued a technical correction in March 2026 clarifying that 92628 and 92631 can be billed on the same date of service if the time requirements for each are independently met and the services did not occur within the same 30-minute window. This correction is retroactive to January 1, 2026.
Stage 3: Fitting and Follow-Up Services (92634 through 92637)
| CPT Code | Service Description | Time | Medicare Covered? |
| 92634 | Hearing device fitting services; first 60 minutes | Base code, 60 min | No |
| 92635 | Hearing device fitting services; each additional 15 min (add-on) | +15 min | No |
| 92636 | Hearing device follow-up; first 30 min | Base code, 30 min | No |
| 92637 | Hearing device follow-up; each additional 15 min (add-on) | +15 min | No |
For 92634, you need 31 to 67 minutes of documented service time to bill the base code. At 68 minutes and beyond, you start billing 92635 for each additional 15-minute increment.
CMS established a Medically Unlikely Edit of 2 units, with an MUE Adjudication Indicator of 3, per date of service, for the add-on codes 92629, 92632, 92635, and 92637. Claims billing more than 2 add-on units on a single date will be flagged. If the service genuinely ran that long, your documentation needs to hold up under review.
Stage 4: Verification Services (92638 through 92642)
| CPT Code | Service Description | Time | Medicare Covered? |
| 92638 | Real-ear measurement verification (add-on) | Untimed | No |
| 92639 | Speech mapping or sound-field verification (add-on) | Untimed | No |
| 92641 | Electroacoustic analysis verification | Per payer guidance | No |
| 92642 | Additional verification services | Per payer guidance | No |
Codes 92638 and 92639 are untimed add-on codes. That means the half-plus-one rule does not apply to them. They are reported in conjunction with the fitting or follow-up codes from the 92634-92637 family to capture the specific verification work performed during or after fitting.
Why Medicare covers None of These New Codes
Here is the part of the 2026 changes that frustrates many audiologists, and rightfully so. Despite all the work that went into modernizing these codes, CMS confirmed in the 2026 final rule that it lacks legal authority to pay for hearing devices or related services under Medicare. Section 1862(a)(7) is the statutory wall. Congress would have to change the law to change that reality.
Because these codes are excluded from Medicare, they have no Relative Value Units assigned in the MPFS.
They never went through the AMA RUC process. For Medicare patients, these services remain either private pay or covered through supplemental insurance plans.
The upside is that without CMS pricing constraints, audiologists have more flexibility to negotiate rates for these services directly with commercial payers, Medicare Advantage plans, employer health plans, and state Medicaid programs that do cover hearing services. ASHA and AAA are both actively working to push commercial and Medicaid payers to adopt the new code set and establish fair payment rates.
MIPS and Quality Reporting for Audiologists in 2026
Most audiologists are still exempt from mandatory MIPS reporting in 2026. To be a mandatory MIPS Eligible Clinician, you need to exceed the low-volume threshold on all three criteria simultaneously: more than $10,000 in Part B allowed charges, more than 100 Medicare patients, and more than 200 distinct procedures within the performance period.
If you fall below any one of those thresholds, you are excluded from mandatory participation. Voluntary reporting is still available, and audiologists who do meet the criteria should be aware that CMS removed two Social Determinants of Health measures from the quality reporting measure sets for 2026, though the overall quality measure library remains robust.
Telehealth: Two Audiology Codes Added to the Covered List
CMS added CPT codes 92622 and 92623, which cover auditory osseointegrated sound processor services, to the Medicare Telehealth Services list for 2026. For practices that see patients with bone-anchored hearing systems, this is a real billing opportunity for follow-up and programming visits that can be conducted via secure telehealth platforms without requiring in-person attendance.
This addition is part of a broader CMS trend to expand telehealth access for audiology services when physical presence is not clinically essential.
What Audiology Practices Must Do Right Now?
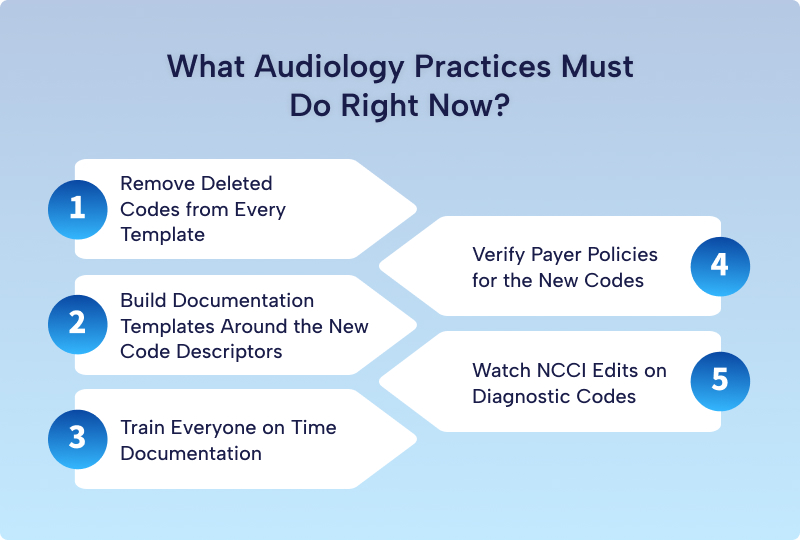
Step 1: Remove Deleted Codes from Every Template
CPT codes 92590 through 92595 no longer exist. Any claim submitted with those codes will be rejected immediately. Check every EHR template, billing system superbill, and encounter form in your practice. If those codes appear anywhere, pull them today. If your practice management vendor has not already pushed an update, contact them directly.
Step 2: Build Documentation Templates Around the New Code Descriptors
Because the new hearing device codes are time-based and descriptive, your clinical note templates need to reflect these requirements. If you are billing 92628, the note must reflect a review of audiologic function tests, an interpretation of hearing needs, a discussion of candidacy results, treatment counseling, and a written report. The code descriptor is your documentation checklist.
Step 3: Train Everyone on Time Documentation
Time-based billing only works when time is actually documented. Every clinician billing the 92628-92642 code set needs to record the total face-to-face time spent per service, with enough clarity to support unit calculation under the half-plus-one rule. Start and end times, or total minutes per service, are the minimum requirements.
Step 4: Verify Payer Policies for the New Codes
Commercial payers, Medicare Advantage plans, and Medicaid programs did not automatically build pricing or coverage for the new 12 codes just because CMS published them.
Contact each of your major payers directly. Ask whether they have loaded the codes, whether prior authorization applies, and whether any bundling edits affect how you report candidacy and selection services on the same date.
Step 5: Watch NCCI Edits on Diagnostic Codes
The NCCI edit restrictions on diagnostic codes have not changed, but they may cause claim denials.
Billing 92553 and 92556 separately, when 92557 should have been used, constitutes unbundling.
Billing 92550 and 92568 on the same day without the proper modifier and documentation is another common RAC audit finding. Keep your billing team up to date on the pairing rules.
Conclusion
The 2026 hearing services fee schedule changes are significant, but they are manageable if you act early and correctly. The practices that will struggle this year are the ones that kept using deleted codes past January 1, never updated their documentation templates, and assumed commercial payers would automatically load pricing for the new codes.
The practices that will do well are the ones that map every deleted code to its replacement, train clinical staff on time-based documentation, and pick up the phone to verify payer policies before denials start stacking up.
Audiology reimbursement is genuinely complex, and the Medicare exclusion on hearing devices makes it more so. But with the right coding framework and tight documentation habits, your practice can navigate 2026 confidently. If you need help auditing your current billing processes or renegotiating commercial payer contracts under the new code structure, that is exactly the kind of work a good RCM partner can help you with.
Need Help Managing Audiology Billing and Coding?
The 2026 audiology fee schedule changes introduce new CPT codes, updated documentation requirements, reimbursement adjustments, and payer policy challenges. RCM Xpert helps audiology clinics, hearing centers, ENT practices, and multi-specialty providers stay compliant while maximizing revenue.
Our Audiology Billing Services Include:
✔ Audiology CPT Coding Support
✔ Medicare & Commercial Claims Management
✔ Denial Prevention & Appeals
✔ Fee Schedule Analysis
✔ Revenue Cycle Management
✔ Documentation Audits
✔ Credentialing & Enrollment Support
Partner with RCM Xpert to improve claim accuracy, reduce denials, and optimize reimbursement under the new 2026 audiology coding framework.