The ICD-10 code for Type 2 diabetes is E11. It is the ICD-10-CM category for Type 2 diabetes mellitus, and it is rarely billed on its own. A fourth or fifth character indicates to the payer exactly what is happening with the patient, ranging from E11.9 for diabetes without complications to E11.22 for diabetic chronic kidney disease.
That specificity is where claims are won or lost. Pick the wrong character, skip a required secondary code, or fail to link the complication to the diabetes in the documentation, and the claim lands in the denial pile.
ICD-10-CM also sets a default worth memorizing: if the provider documents diabetes without specifying the type, the coder assigns Type 2. E11 is the default category, which makes it one of the most frequently billed diagnosis families in outpatient medicine.
This guide covers the full E11 code family, including the new E11. A remission code that took effect on October 1, 2025, the secondary code payers expect alongside each complication, and the documentation rules that keep your claims clean.
E11 Codes at a Glance: Quick Reference Table
Here is every code covered in this guide in one place. The third column is the part most coders miss: several E11 codes are invalid or incomplete without a secondary code on the claim.
| Code | Descriptor | Required or Common Secondary Code |
|---|---|---|
| E11.9 | Type 2 diabetes without complications | Z79.4, Z79.84, or Z79.85 if on long-term medication |
| E11.A | Type 2 diabetes in remission (new October 1, 2025) | None; provider must document remission |
| E11.8 | Type 2 diabetes with unspecified complications | Avoid when the complication is identifiable |
| E11.00 / E11.01 | With hyperosmolarity, without / with coma | None |
| E11.10 / E11.11 | With ketoacidosis, without / with coma | None |
| E11.21 | With diabetic nephropathy | None unless a CKD stage is documented |
| E11.22 | With diabetic chronic kidney disease | N18.1 to N18.6, or N18.9 (required) |
| E11.29 | With other diabetic kidney complication | Code the specific condition if named |
| E11.319 | With unspecified retinopathy, without macular edema | H54.x if visual impairment is documented |
| E11.36 | With diabetic cataract | None |
| E11.40 / .41 / .42 / .43 | Neuropathy: unspecified / mono / poly / autonomic | None |
| E11.51 | With diabetic peripheral angiopathy | None; I73.x is excluded (Excludes1) when the angiopathy is diabetic |
| E11.52 | With gangrene | L97.x if an ulcer is present; never add I96 (Excludes1) |
| E11.621 | With foot ulcer | L97.4x or L97.5x for site, laterality, depth (required) |
| E11.622 | With other skin ulcer | L97.x or L98.4x for the site (required) |
| E11.65 | With hyperglycemia | None |
| E11.649 / E11.641 | With hypoglycemia, without / with coma | None |
| Z79.4 / Z79.84 / Z79.85 | Long-term insulin / oral agents / injectable non-insulin agents | Always secondary to an E11 code |
The E11 Code Family: Your Starting Point
First things first. All Type 2 diabetes codes start with E11. This is the category for Type 2 diabetes mellitus.
What makes ICD-10 different from the old ICD-9 system is that it is much more detailed. The codes are combination codes. This means one code can capture the type of diabetes, the body system affected, and the specific complication.
If you do not specify the type, the default is Type 2. So, if you document “diabetes” without saying Type 1 or Type 2, the coder has to use E11. That is a good default, but it is not always the most accurate.
The Foundation: E11.9 – Without Complications
The most basic code in this family is E11.9. This stands for Type 2 diabetes mellitus without complications.
You use this code when the patient has Type 2 diabetes, but there are no documented complications from the disease. There is no neuropathy, no nephropathy, no retinopathy. The patient might be managing their condition with diet, exercise, or medication, but they have not developed any of the classic diabetes-related issues.
Example: A 52-year-old man comes in for a three-month follow-up. His diabetes is well controlled with Lantus, diet, and exercise. He has no complaints. The provider refers him for a routine diabetic eye exam. There are no other issues documented. The correct code is E11.9.
E11.9 is one of the most frequently reported diagnosis codes in primary care and endocrinology, and that popularity is exactly why payers watch it. An easy default becomes an easy audit target.
One habit protects you here: make sure the note shows that complications were assessed and ruled out, not just left unmentioned. A chart that is silent on complications and a chart that confirms their absence look identical to a coder, but they look very different to a payer reviewing medical necessity. A single line such as “no signs of retinopathy, nephropathy, or neuropathy” turns E11.9 from an assumption into a supported diagnosis.
E11.9 vs E11.8 vs E11.A: Choosing the Right Default Code
E11.9 means no complications are documented, E11.8 means a complication exists but is not specified, and E11.This means the diabetes is in documented remission. These three codes describe three different patients, and mixing them up is a fast route to denials and audit flags.
| Code | When to Use It | Documentation Example |
|---|---|---|
| E11.9 | No complications documented; routine management of active Type 2 diabetes | “Type 2 diabetes, stable on metformin, no complications noted” |
| E11.8 | The provider states a complication exists but does not identify it. Use sparingly; it invites payer scrutiny | “Type 2 diabetes with complications” and nothing more specific anywhere in the note |
| E11.A | The provider explicitly documents remission: normal glucose sustained without diabetes medication | “Type 2 diabetes in remission following bariatric surgery, A1c 5.9%, off all agents” |
If the note names the complication anywhere, skip E11.8 and code the specific complication. If the note says the diabetes has “resolved”, do not reach for E11.A yet. That word has a specific problem we cover next.
E11.A: Type 2 Diabetes in Remission (New for 2026)
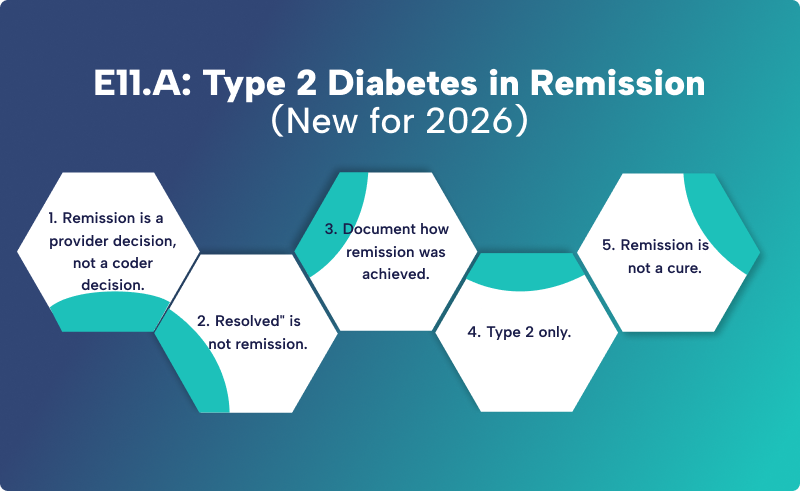
E11.A is the ICD-10-CM code for Type 2 diabetes mellitus without complications in remission, effective October 1, 2025. It reports patients with a confirmed history of Type 2 diabetes who have maintained an A1c below 6.5% for at least 3 consecutive months without taking any glucose-lowering medication.
Before this code existed, coders had no accurate option for these patients. E11.9 overstated the disease as active, and dropping the diagnosis entirely erased a clinically important history. E11. A close that gap, and it aligns with the American Diabetes Association consensus definition of remission.
The rules that trip people up:
- Remission is a provider decision, not a coder decision. You cannot assign E11. Just because the A1c values in the chart have been normal for months. The provider must state that the diabetes is in remission. If they have not, query.
- Resolved” is not remission. The ICD-10-CM Official Guidelines are explicit that the term “resolved” is not synonymous with remission. If the note says resolved, query the provider before assigning E11.A.
- Document how remission was achieved. Strong notes name the intervention: sustained weight loss through diet and exercise, a supervised weight loss program, bariatric surgery, or a combination.
- Type 2 only. E11.A never applies to Type 1 diabetes, drug-induced diabetes, or diabetes due to an underlying condition.
- Remission is not a cure. Relapse is possible, so ongoing monitoring visits, A1c checks, and lifestyle counseling remain appropriate and billable. E11.A supports follow-up care rather than ending it.
Example: a 49-year-old patient diagnosed with Type 2 diabetes 4 years ago undergoes bariatric surgery and loses 60 pounds. Her A1c has stayed below 6.5% for 9 months with no diabetes medication. The provider documents “Type 2 diabetes in remission following bariatric surgery.” Code E11.A.
E11.0 and E11.1: Hyperosmolarity and Ketoacidosis
The acute metabolic emergencies of Type 2 diabetes sit at the top of the code family. E11.00 reports Type 2 diabetes with hyperosmolarity without coma, and E11.01 reports it with coma. E11.10 reports Type 2 diabetes with ketoacidosis without coma, and E11.11 reports it with coma.
The common error is habit: many coders still associate diabetic ketoacidosis (DKA) with Type 1 diabetes and reflexively reach for an E10 code. DKA occurs in Type 2 patients too, and when it does, the E11.1 codes are correct. Code the type the provider documented, not the type the textbook expects.
The Next Level: Codes for Specific Complications
When a patient has diabetes-related complications, you need to use a more specific code. Here is where it gets detailed.
Kidney Complications (E11.21 and E11.22)
Diabetes is a leading cause of kidney disease. If your patient has diabetic nephropathy or chronic kidney disease related to their diabetes, you use the E11.2 family.
- E11.21 is for Type 2 diabetes with diabetic nephropathy. This is the classic kidney complication.
- E11.22 is for Type 2 diabetes with diabetic chronic kidney disease. This is used when the patient has CKD that is specifically due to their diabetes.
Important: When you use E11.22, you must add code to identify the stage of the CKD. This is not optional. Use codes N18.1 through N18.6 to indicate the stage.
Example: A patient has Type 2 diabetes and diabetic chronic kidney disease, stage 3. You would use E11.22 and N18.3.
The series has a third member: E11.29, for other diabetic kidney complications. Use it when kidney involvement is documented and linked to the diabetes, but does not fit nephropathy or staged CKD, such as an early diabetic renal disorder that the provider has not classified further.
Two more details keep this series clean. If the CKD stage is not documented, E11.22 still requires a secondary code, so use N18.9 (CKD, unspecified) and flag the chart for a provider query. If the patient has end-stage renal disease, the stage code is N18.6, and dialysis status should be coded when documented. And if the note says “nephropathy” without any diabetic link, do not assume: query the provider. “Diabetic nephropathy” supports E11.21; a bare “nephropathy” does not.
Neurological Complications (E11.40, E11.42)
Diabetes often damages nerves. This is called diabetic neuropathy. There are a few codes in this family.
- E11.40 is for diabetic neuropathy, unspecified. Use this when the provider documents neuropathy but does not specify the type.
- E11.42 is for diabetic polyneuropathy. This is the most common type of diabetic neuropathy, affecting multiple nerves. It is often documented simply as “diabetes with polyneuropathy”.
- E11.43 is for diabetic autonomic neuropathy. This affects the autonomic nervous system and can cause gastroparesis, among other issues.
Example: A patient has Type 2 diabetes with diabetic polyneuropathy. The provider documents “diabetes with polyneuropathy.” You would use E11.42.
E11.4 Series: Neuropathy Codes (E11.40 to E11.43
E11.41 is for diabetic mononeuropathy, meaning a single nerve is involved rather than a symmetrical pattern. Think diabetic cranial nerve palsy or an isolated median or ulnar nerve lesion documented as diabetic in origin. It is far less common than polyneuropathy, which is why it gets skipped, and why using E11.40 when the note clearly says “mononeuropathy” is an avoidable specificity miss.
E11.3 Series: Eye Complications and Diabetic Retinopathy
The E11.3 series codes for diabetic eye disease and is the most granular series in the family. A complete retinopathy code answers 4 questions: is the retinopathy nonproliferative or proliferative, how severe is it, is macular edema present, and which eye is affected.
When the documentation answers none of those questions, E11.319 is the workhorse: Type 2 diabetes with unspecified diabetic retinopathy without macular edema. It is the most common retinopathy code on claims for exactly that reason.
When the documentation is detailed, the series rewards it. Mild, moderate, and severe nonproliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy each have their own subcategory. A sixth character reports whether macular edema is present, and a seventh character reports laterality: right eye, left eye, or bilateral. Code to the highest level of specificity the note supports, and query the ophthalmologist when a report mentions severity but omits laterality.
Two companions round out the series. E11.36 reports Type 2 diabetes with diabetic cataract. And when retinopathy has caused documented visual impairment, add an H54. x code to report the level of vision loss alongside the E11.3 code.
Example: the ophthalmology note reads “moderate NPDR, right eye, without macular edema, due to Type 2 diabetes.” That documentation supports a fully specified code from the moderate NPDR subcategory with the right-eye seventh character, not E11.319. Detailed notes deserve detailed codes; that specificity is what survives an audit.
E11.5 Series: Circulatory Complications
The E11.5 series codes the vascular damage caused by diabetes, and it is the series most often missing from claims involving diabetic foot disease. There are 3 codes.
E11.51 is for Type 2 diabetes with diabetic peripheral angiopathy without gangrene. Use it when the provider documents peripheral arterial disease (PAD), peripheral vascular disease, or vascular insufficiency as diabetic in origin. Do not add I73.9 alongside it: I73.9 carries an Excludes1 note for diabetic peripheral angiopathy, which means the two codes can never appear together. The combination code stands alone. You will find billing guides online that instruct pairing E11.51 with I73.9; that advice fails the Excludes1 edit.
E11.52 is for Type 2 diabetes with diabetic peripheral angiopathy with gangrene. The same trap repeats here: I96 (gangrene, not elsewhere classified) has an Excludes1 note for gangrene in diabetes, so E11.52 plus I96 is a non-compliant pair. The gangrene is already built into E11.52. What the claim often needs is an L97.x code when an ulcer is present, coded to site, laterality, and depth.
E11.59 is for other circulatory complications, the catch-all for documented diabetic vascular involvement that is neither classic peripheral angiopathy nor gangrene, such as diabetic microangiopathy.
One caution:
The diabetic link still matters here. If a patient’s PAD is attributed to smoking rather than diabetes, E11.51 is wrong. Code the diabetes and the PAD separately unless the provider connects them.
E11.6 Series: Skin and Ulcer Complications
This is a big one. Diabetes is a major cause of foot ulcers. The code E11.621 is for Type 2 diabetes with foot ulcer.
When you use this code, you must add code to specify the site of the ulcer. Use codes from the L97 family for this.
Example: a patient has a left heel ulcer with skin breakdown due to Type 2 diabetes. You would use E11.621 and L97.421. If the note only said left foot without naming the heel or midfoot, the site code would come from L97.5 instead, the subcategory for other parts of the foot.
The L97 code is doing 3 jobs at once: it reports the site (heel and midfoot codes live in L97.4, other parts of the foot in L97.5), the laterality (right or left), and the depth (limited to skin breakdown, fat layer exposed, necrosis of muscle, or necrosis of bone). The final character is the depth, so an ulcer code ending in 9 tells the payer the severity was not documented. That is a documentation gap worth querying, because depth drives both clinical urgency and reimbursement.
E11.622 covers Type 2 diabetes with other skin ulcers, for diabetic ulcers that are not on the foot. It carries the same instruction: add the site code from L97. x or L98.4x.
And one trap: pressure ulcers are not diabetic ulcers. If the wound is documented as a pressure injury, the site code comes from L89.x with its staging system, not L97.x. Using L97 for a pressure ulcer is one of the most common wound-coding errors on diabetic charts.
ICD-10 Code for Type 2 Diabetes With Hyperglycemia and Hypoglycemia (E11.65, E11.649)
You cannot use “controlled” or “uncontrolled” in ICD-10. Those terms are not part of the coding system. Instead, you use hyperglycemia or hypoglycemia.
- E11.65 is for Type 2 diabetes with hyperglycemia.
- E11.649 is for Type 2 diabetes with hypoglycemia without coma.
Example: A patient’s diabetes is poorly controlled, and they have hyperglycemia. The provider documents “diabetes mellitus Type 2, poorly controlled.” You would code this as E11.65.
Hypoglycemia has a second code: E11.641, Type 2 diabetes with hypoglycemia with coma. E11.649 covers hypoglycemia without coma; if the patient lost consciousness, E11.641 is the accurate choice.
There is also a boundary to respect. E11.65 requires a diabetes diagnosis. If a patient has elevated blood glucose but no diagnosed diabetes, the code is R73.9 (hyperglycemia, unspecified) or another R73 code, never E11.65. Coding diabetes that has not been diagnosed is a compliance problem, not a shortcut.
E10 vs E11 vs E13: Coding the Right Type of Diabetes
E11 is only correct when the patient has Type 2 diabetes or the type is not documented. ICD-10-CM separates diabetes into distinct categories, and picking the wrong one misstates the patient’s clinical picture.
| Category | Covers | Note |
|---|---|---|
| E10 | Type 1 diabetes mellitus | Never assign Z79.4 with E10; insulin use is inherent to the condition |
| E11 | Type 2 diabetes mellitus | The default when the type is not documented |
| E13 | Other specified diabetes mellitus | Genetic defects, post-pancreatectomy, other specified forms |
| E09 | Drug- or chemical-induced diabetes | For example, steroid-induced diabetes; code the drug too |
| O24 | Diabetes in pregnancy, including gestational | Obstetric chapter codes take sequencing priority |
The complication logic works the same way across categories, so everything in this guide about fourth and fifth characters transfers. What does not transfer is the type itself: if the provider documents Type 1, autoimmune, or drug-induced diabetes, an E11 code is wrong, no matter how well the complication characters match.
Prediabetes: When Not to Use an E11 Code
The ICD-10 code for prediabetes is R73.03, not anything in the E11 family. Prediabetes means glucose levels above normal but below diagnostic thresholds for diabetes, and coding it as E11 is overcoding with real consequences: it plants a chronic diagnosis in the patient’s record that payers, underwriters, and future providers will treat as established disease.
Two neighbors complete the boundary. R73.9 reports hyperglycemia, unspecified, for elevated glucose findings without a diabetes or prediabetes diagnosis. Z13.1 reports an encounter for diabetes screening in an asymptomatic patient. Keep all 3 in your toolkit and the E11 family stays reserved for what it actually means: diagnosed Type 2 diabetes.
Key Documentation Rules for Type 2 Diabetes ICD 10 Codes
Coding is only as good as the documentation. If the provider does not write it down, the coder cannot code it. Here are the rules that keep claims out of the denial pile.
Rule 1: Link the Complication to the Diabetes
The complication codes are combination codes. They are designed to link the complication directly to the diabetes. The provider’s documentation must show this relationship.
Look for words like “due to,” “associated with,” or “diabetic.” For example, “CKD stage IV due to diabetic nephropathy” clearly links the CKD to the diabetes.
If the provider does not link the two conditions, you cannot use the combination code. You have to code them separately.
Example of incorrect coding: A female patient has Type 1 diabetes and stage 1 CKD. The provider documents both conditions but does not state that the CKD is due to the diabetes. You cannot use a combination code. You would use E10.9 for the diabetes and N18.1 for the CKD.
Rule 2: Document Hyperglycemia or Hypoglycemia, not “Controlled” or “Uncontrolled”
ICD-10 eliminated the use of “controlled” and “uncontrolled” for diabetes. Instead, you need to document whether the patient has hyperglycemia or hypoglycemia.
If the patient’s diabetes is not well controlled, the provider should document “hyperglycemia.” If the patient’s blood sugar is too low, they should document “hypoglycemia.”
Rule 3: Code Diabetes Annually
Even if the diabetes is well managed, you need to code it at least once a year. This is important for tracking the patient’s condition and for quality metrics.
Rule 4: Use Additional Codes for Medication Use
Z-codes tell the payer how the diabetes is being managed, and they are expected on the claim whenever long-term therapy is documented. There are 3:
- Z79.4 for long-term (current) use of insulin.
- Z79.84 for long-term (current) use of oral hypoglycemic drugs, such as metformin, sulfonylureas, or SGLT2 inhibitors.
- Z79.85 for long-term (current) use of injectable non-insulin antidiabetic drugs, which is where GLP-1 receptor agonists such as semaglutide belong. With GLP-1 prescribing at record levels, this is now one of the most frequently missed codes on diabetes claims.
Assign the codes for the therapies the patient is actually on, in combination, when the documentation supports it. A patient managed with metformin and long-term insulin gets both Z79.84 and Z79.4. A patient on insulin plus a weekly GLP-1 injection gets Z79.4 and Z79.85. The old habit of reporting only the insulin code when oral agents were also in use came from guideline language that has since been revised; do not carry it forward.
One exception stands: never assign Z79.4 with Type 1 diabetes. Insulin use is inherent to Type 1 and does not get a separate code.
Rule 5: Make Every Note Pass the MEAT Test
Payers and risk-adjustment auditors evaluate diabetes documentation against the MEAT criteria: the note must show the condition was Monitored, Evaluated, Assessed, or Treated during the encounter. A diagnosis that just sits in the problem list without any of the 4 does not support the code.
A compliant note does not need to be long. This one line covers all 4 letters: “Type 2 diabetes, A1c 6.8% reviewed today, stable on metformin 1000 mg twice daily, no signs of retinopathy, nephropathy, or neuropathy; continue current regimen, recheck A1c in 3 months.” Monitoring is the A1c check, evaluation is the review, assessment is the stability statement, and treatment is the medication plan. Build that habit into templates, and the MEAT problem disappears.
Why Specificity Pays: Diabetes and HCC Risk Adjustment
Diabetes coding does not just decide whether a single claim pays. Under Medicare Advantage and other value-based programs, diagnosis codes feed Hierarchical Condition Categories (HCCs), and diabetes with chronic complications maps to a higher-weighted category than uncomplicated diabetes.
That means every time a patient with documented diabetic CKD or neuropathy is coded E11.9, the practice is not just risking a denial. It is understating the patient’s risk adjustment factor (RAF), which understates the capitated revenue the plan receives for that patient’s care. Multiply one habitual undercode across a diabetic panel, and the annual revenue impact is substantial, and completely invisible on any single claim.
The fix is the same discipline this whole guide teaches: code every documented complication to its full specificity, every year, with the linking language in place. Accurate HCC capture is a documentation outcome, not a billing trick.
Common Mistakes and How to Avoid Them
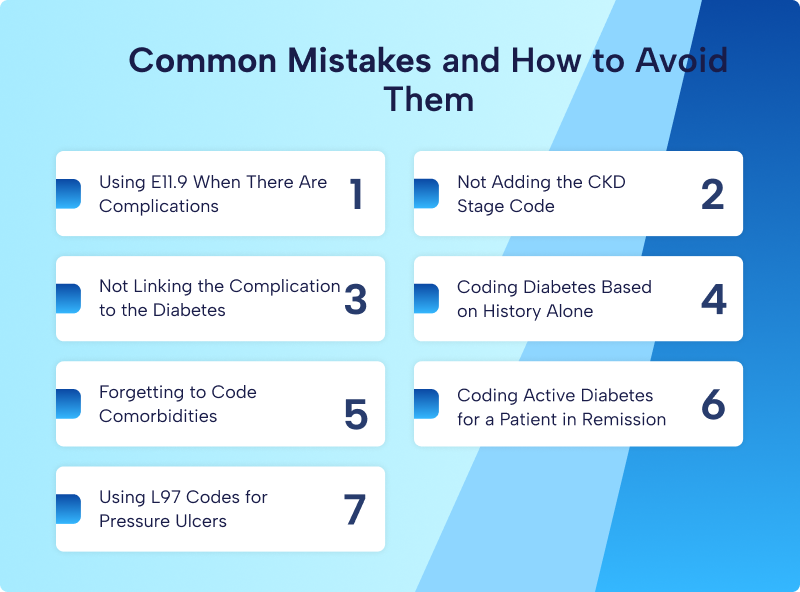
There are a few common errors that cause claims to be denied. Here is how to avoid them.
Mistake 1: Using E11.9 When There Are Complications
This is the most common mistake. E11.9 is for “without complications.” If the patient has neuropathy, nephropathy, or any other complication, you cannot use E11.9.
How to avoid it: Read the documentation carefully. If you see any complication, use the appropriate specific code.
Mistake 2: Not Adding the CKD Stage Code
E11.22 requires an additional code for the CKD stage. If you do not add it, the claim will deny.
How to avoid it: Always include N18.1 through N18.6 when you use E11.22.
Mistake 3: Not Linking the Complication to the Diabetes
If the provider documents CKD but does not link it to the diabetes, you cannot use E11.22. You must code them separately.
How to avoid it: Review the documentation for linking verbiage. If it is not there, use separate codes.
Mistake 4: Coding Diabetes Based on History Alone
A patient might tell you they have diabetes, but that does not mean you can code it. You need documented diagnostic criteria in the chart for the current encounter.
How to avoid it: Only code diabetes if there is a confirmed diagnosis in the chart.
Mistake 5: Forgetting to Code Comorbidities
Patients with diabetes often have hypertension, hyperlipidemia, and obesity. Each of these requires its own code.
How to avoid it: Review the chart for all comorbidities and code them all. Do not just stop at the diabetes code.
Mistake 6: Coding Active Diabetes for a Patient in Remission
Since October 1, 2025, a patient whose provider has documented remission should be coded E11.A, not E11.9. Coding E11.9 overstates active disease and contradicts the record. The reverse error matters too: do not assign E11. A without an explicit provider statement of remission, and remember that “resolved” does not count.
Mistake 7: Using L97 Codes for Pressure Ulcers
L97.x is for non-pressure chronic ulcers, the classic diabetic ulcer. If the wound is documented as a pressure injury, the site and stage come from L89.x. Swapping the two misrepresents the wound type and the required staging detail, and wound care claims get reviewed closely enough that this one rarely slips through.
| A Real-World Example for Correct and Incorrect Coding
A 55-year-old patient with Type 2 diabetes presents for a follow-up. They have chronic diabetic kidney disease, stage 3. They are on insulin. There are no other complications. Correct Coding:
Incorrect Coding:
|
A Second Example: Coding Remission Correctly
A 49-year-old patient diagnosed with Type 2 diabetes 4 years ago has maintained an A1c below 6.5% for 9 months following bariatric surgery, with no diabetes medication. The provider documents “Type 2 diabetes in remission.”
Correct coding: E11.A, Type 2 diabetes mellitus without complications in remission. No Z79 code, because the patient is not on long-term therapy.
Incorrect coding: E11.9 (the diabetes is not active), or dropping the diabetes diagnosis entirely (the history is clinically significant and supports the ongoing monitoring visits).
The Bottom Line
E11 coding for Type 2 diabetes is not complicated once you understand the rules. The key is specificity. Document the type of diabetes.
Document any complications. Link the complications to diabetes. Add any required additional codes.
And never use E11.9 when there are complications.
Get these pieces right, and your claims will pay. Get them wrong, and you will be dealing with denials and lost revenue.
Frequently Asked Questions
What is the default ICD-10 code for Type 2 diabetes?
The default code is E11.9 for Type 2 diabetes mellitus without complications. This is the code to use when the provider documents “diabetes” without specifying Type 1 or Type 2, and there are no documented complications.
Can I use E11.9 for a patient with diabetes and other conditions?
No. E11.9 is only for Type 2 diabetes without complications. If the patient has any complication, like neuropathy or nephropathy, you need to use a different, more specific code from the E11 family.
What code should I use for Type 2 diabetes with CKD?
Use E11.22 for Type 2 diabetes with diabetic chronic kidney disease. You must also include a secondary code from N18.1 through N18.6 to indicate the stage of the CKD. For example, E11.22 and N18.3 for stage 3 CKD.
How do I code “uncontrolled” Type 2 diabetes?
You do not use the terms “controlled” or “uncontrolled” in ICD-10. Instead, you code based on the specific manifestation. If the patient has high blood sugar, use E11.65 for hyperglycemia. If they have low blood sugar, use E11.649 for hypoglycemia without coma.
Do I need to code the medications a patient takes for diabetes?
Yes. Use Z79.4 for long-term insulin, Z79.84 for oral hypoglycemic drugs, and Z79.85 for injectable non-insulin agents such as GLP-1 receptor agonists. Assign them in combination when the patient is on more than one therapy, for example, Z79.4 plus Z79.84 for a patient on insulin and metformin.
What is the ICD-10 code for type 2 diabetes with hyperglycemia?
E11.65 is the ICD-10 code for Type 2 diabetes with hyperglycemia. Documentation of “uncontrolled” or “poorly controlled” diabetes maps here, because ICD-10-CM does not use those terms. If the patient has high glucose but no diabetes diagnosis, use R73.9 instead.
What is the new ICD-10 code for diabetes in remission?
E11.A, effective October 1, 2025, reports Type 2 diabetes in remission. It applies when the provider documents remission, typically an A1c below 6.5% sustained for at least 3 months without glucose-lowering medication. The provider must state remission; normal labs alone are not enough.
What is the difference between E11.8 and E11.9?
E11.9 means no complications are documented. E11.8 means the provider documented a complication but never identified it. Use E11.8 conservatively: if the complication is named anywhere in the record, code it specifically, because unspecified-complication claims draw payer scrutiny.
What is the ICD-10 code for prediabetes?
R73.03 is the ICD-10 code for prediabetes. It is not part of the E11 family, and coding prediabetes as diabetes is overcoding. For elevated glucose without a diagnosis, use R73.9, and for diabetes screening encounters, use Z13.1.
What is the ICD-10 code for diabetic ketoacidosis in type 2 diabetes?
E11.10 reports Type 2 diabetes with ketoacidosis without coma, and E11.11 reports it with coma. DKA is not exclusive to Type 1 diabetes, so code the type the provider documented rather than defaulting to an E10 code.
Ready to Simplify Your Diabetes Coding?
Diabetes coding is complex, and denials are costly. If you are spending too much time fixing coding errors or chasing denied claims, it may be time to get help.
At RCM Xpert, we specialize in medical coding and revenue cycle management for practices of all sizes. Our certified medical coders stay on top of ICD-10-CM updates, payer requirements, and documentation standards so you do not have to, including this year’s changes like the new E11.A remission code.
We make sure your claims are coded accurately the first time, so you get paid faster and spend less time on administrative headaches.